What is Trauma
Trauma is similar to memory
cells in the immune system, the brain and nervous system become sensitised to subsequent stressful or perceived stressful events experienced via neuroception as threatening or even life threatening mirroring an original experience or experiences once faced in early childhood. Memory T and B lymphocytes have an essential role in the immunity against microbial pathogens. Immunological memory occurs after a primary immune response against the antigen. Immunological memory is thus created by each individual, after a previous initial exposure, to a potentially dangerous agent. The course of secondary immune response is similar to primary immune response. After the memory B cell recognizes the antigen it presents the peptide: MHC I complex to nearby effector T cells. That leads to activation of these cells and rapid proliferation of cells. After the primary immune response has disappeared, the effector cells of the immune response are eliminated. However, there remain antibodies previously created in the body that represent the humoral component of immunological memory and comprise an important defensive mechanism in subsequent infections. In addition to the formed antibodies in the body there remains a small number of memory T and B cells that make up the cellular component of the immunological memory. They stay in blood circulation in a resting state and at the subsequent encounter with the same antigen these cells are able to respond immediately and eliminate the antigen. Memory cells have a long life and last up to several decades in the body. When there has been chronic inflammation, chronic infections or chronic stress/anxiety induced burden on this immune response, these memory cells become overactive and start to attack friendly cells and organs confusing them for threats, this is autoimmunity and presents in syndromes such as IBS, IBD, Colitis etc. The trauma impacted brain and nervous system acts in a very similar way to immune system memory cells responding to subsequent threat or perception of treat which happens below conscious awareness through a process called neuroception. In traumatology this is called sensitised. After a traumatic event or encounter we become sensitised to a look, a sound, a smell, a feeling that may represent a cue of the original event. We then act in ways which may not promote prosocial reciprocity, we may appear defensive, mistrusting, angry, even agressive or withdrawn, all theses are the defenses we use to protect us from a repeat of the original trauma whilst co creating a variation of the original trauma via reenactment. The road to a healthy secure relationship is usually extremely difficult for people who have experienced neglect and trauma precisely because the defenses we use to avoid the painful past often wind up provoking it's recreation in the present setting up a perpetual cycle of toxic stress, inflammation and adversity.
Childhood trauma has profound impact on the emotional, behavioral, cognitive, social, and physical functioning of children. Developmental experiences determine the organizational and functional status of the mature brain. There are various adaptive mental ,relational and physical responses to trauma, including physiological hyperarousal and dissociation. Where once these response were adaptive survival states they become maladaptive as we mature. Because the developing brain organizes and internalizes new information in a use-dependent fashion, the more a child is in a state of hyperareusal or dissociation, the more likely they are to have neuropsychiatric symptoms following trauma. The acute adaptive states, when they persist, can become maladaptive traits locking us into a lifelong perpetual cycle of rupture without repair, chaos without relaxation. Life becomes about survival rather than connection.
The Trauma Recovery Institute
Defining Trauma at The Trauma Recovery Institute
The prevailing definition of trauma has been that psychological trauma is a response to an event that a person finds highly stressful. Examples include being in a war zone, a natural disaster, or a serious car accident. We now understand so much more about trauma, its definition and implications and it seems trauma is much broader and more complex than once appreciated, perhaps best seen as a spectrum including adverse childhood experiences, neglect, sexual abuse, violence, bullying and ofcourse attachment trauma. As a trauma specialist at The Trauma Recovery Institute, I hypothesize that infact most of us have experienced some form of trauma or/and adversity growing up evidenced by the prevalence in our society of addictions to food, drugs and alcohol, our difficulty as a society to maintain healthy long term romantic relationships and our overwhelming health crisis due to poor lifestyle choices. Once seen as all very separate societal challenges, now it is difficult to separate any of the above from adverse childhood experiences. Our childhood is the critical period for brain development which is shaped by experience, experiences become our biology and so dictates how we engage in the world later on, largely governing the choices we make, the relationships we enter into or choose not to, how skilled we are in those relationships including romantic and parental and our relationship to our physical and mental health.
The DSM-5 definition of trauma requires
actual or threatened death, serious injury, or sexual violence”. Stressful events not involving an immediate threat to life or physical injury such as psychosocial stressors (e.g., divorce or job loss) are not considered trauma in this definition. The general definition is, trauma can be defined as a psychological, emotional response to an event or an experience that is deeply distressing or disturbing. ... However, it can also encompass the far extreme and include experiences that are severely damaging, such as rape or torture. Another trauma specialist Bob Scaer defines trauma as A life-threatening experience, either ‘real’ or imagined, may also become a traumatic experience if it occurs in a state of helplessness. Bessell van Der Kolk, a trauma clinician defines trauma as specifically an event that overwhelms the central nervous system, altering the way we process and recall memories. Trauma is not the story of something that happened back then, It's the current imprint of that pain, horror, and fear living inside people. Other trauma researchers suggest that infect it is not the events or events that are defined as trauma but Trauma is what lives on after a traumatic event or events. As you can see there are many ways to define trauma, from a clinical perspective the most beneficial definition in my opinion is looking at what is the impact of traumatic experiences on todays body, mind and relationships. Trauma will infiltrate all areas of our life and show up in often very challenging ways, these challenges provided windows into the impact of previous traumatic experiences and give suggestion as to what corrective experience may be needed. This is the complex work of trauma recovery
We use our minds not to discover facts but to hide them. One of things the screen hides most effectively is the body, our own body, by which I mean, the ins and outs of it, its interiors. Like a veil thrown over the skin to secure its modesty, the screen partially removes from the mind the inner states of the body, those that constitute the flow of life as it wanders in the journey of each day. The elusiveness of emotions and feelings is probably . . . an indication of how we cover to the presentation of our bodies, how much mental imagery masks the reality of the body”
Damasio
The effect of the experience
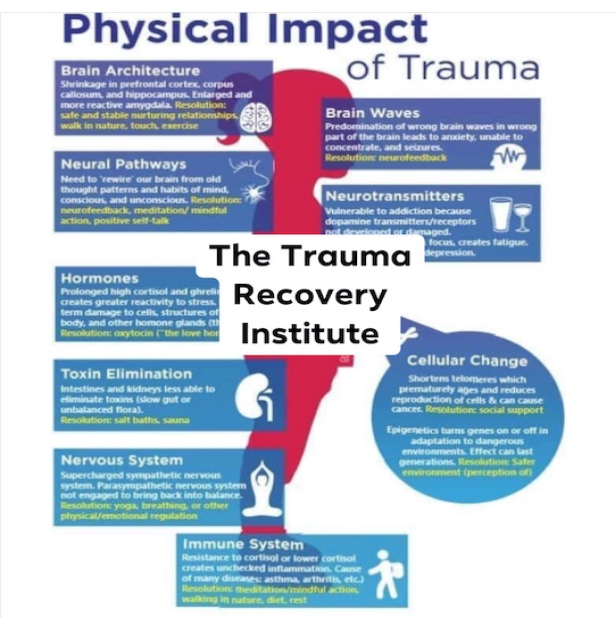
The effect of the experience of trauma over the life span lays the seeds for most chronic, poorly understood disease processes that defy explanation by our current concepts of health and disease.
These chronic diseases make up the majority of symptoms for which patients present to doctor’s offices. The brain, mind, and body exist on a continuum, wherein sensory input from the body shapes and changes the structure and function of the brain, which concurrently shapes and alters the body in all of its parts -- particularly those that provided the sensory input to the brain. The brain and body are intimately inter- related rather than two distinct parts of the greater whole. These two parts of the continuum form a dynamically changing nervous system, constantly and reciprocally adapting based on the influence of the other. The mind is a receptacle for perceptual experience, including body sensations or feelings, and the positive or negative emotions that are related to that information.
The mind is based on brain activity and is the conscious manifestation of what we sense and feel based on the dynamic interaction of the brain / body. Trauma can be conceptualized as stemming from a failure of the natural physiological activation and hormonal secretions to organize an effective response to threat. Rather than producing a successful fight or flight response the organism becomes immobilized. Probably the best animal model for this phenomenon is that of ‘inescapable shock,” in which creatures are tortured without being unable to do anything to affect the outcome of events. The resulting failure to fight or flight, that is, the physical immobilization (the freeze response), becomes a conditioned behavioral response. The psychobiology of early childhood development involving maturation of orbitofrontal and limbic structures is based on reciprocal experiences with the caregiver we call attunement, the nonverbal reciprocal exchange of safety cues between mother and child. Dysfunctional associations in this dyadic relationship result in permanent physicochemical and anatomical changes, which have implications for personality development as well as for a wide variety of clinical manifestations. An intimate relationship may exist, with negative child/care giver interaction leading to a state of persisting hypertonicity of the sympathetic and parasympathetic systems that may profoundly affect the arousal state of the developing child. Sustained hyperarousal in these children may markedly affect behavioural and characterological development. Many traumatised children and adults, confronted with chronically overwhelming emotions, lose their capacity to use emotions as guides for effective action. They often do not recognize what they are feeling and fail to mount an appropriate response. This phenomenon is called alexithymia, an inability to identify the meaning of physical sensations and muscle activation. Failure to recognize what is going on causes them to be out of touch with their needs, and, as a consequence, they are unable to take care of them. This inability to correctly identify sensations, emotions, and physical states often extends itself to having difficulty appreciating the emotional states and needs of those around them. Unable to gauge and modulate their own internal states they habitually collapse in the face of threat, or lash out in response to minor irritations. Dissociation and/or Futility become the hallmark of daily life.
Trauma & learned responses
Traumatic life experiences often contribute to learned habits of movement and posture that reflect the self-protective movement patterns associated
with those threats. Many of these trauma-related movement patterns affect the way that we move, sit and stand. They may lead to patterns of movement and posture that are abnormal and they may inhibit our normal coordination and our learning of other desirable motor skills.
Self-protective movement and postural patterns of the experienced trauma are stored in the brain and the body’s survival memory. These learned dysfunctional patterns persist because they are, in a metaphorical sense, necessary for defense against future threats similar to those that elicited the defense in the first place. If traumatic memories are implanted in the brain, internal cues (such as dreams, imagined scenarios, and memories) as well as sensory information from the external environment will evoke motor, autonomic, somatic, and visceral responses to a perceived threat. This process is almost entirely unconscious and occurs typically before any conscious recognition or awareness. Using the term ‘psychological’ as opposed to ‘physical’ to explain a physical symptom or somatic feeling state or emotional event defies the obvious – that all perceptions, thoughts, symbols, or experiences have a physiological basis within the mind / body continuum.


Dynamic Psychosocialsomatic Psychotherapy
is grounded in models such as affect regulation theory, an interpersonal neurobiological model of emotional and social development from early human beginnings and across the lifespan, attachment research, polyvagal theory, traumatology and interpersonal neurobiology. Drawing upon these various scientific and clinical disciplines, our trauma recovery work describes how the structure and function of the right mind and brain are indelibly shaped by experiences, especially those embedded in emotional relationships, and how communicating right brains align and synchronize their neural activities with other right brains.
These experiences of interpersonal synchrony are a central focus of Psychosocialsomatic Psychotherapy. At Trauma Recovery Institute we attempt to get to the root of your life challenging symptoms, discomfort, illness and maladaptive behaviours. This is not another talk therapy, we specialise in personality disorders & complex trauma and focus on the brain, body, mind, diet, lifestyle, relationships and most importantly the nervous system of which traumatic experiences have greatly shaped thus priming a predisposition of subsequent adversity. The definition of a traumatic experience is an experience or experiences that overwhlem our capacity to cope. Trauma effects all areas of the brain and all bodily systems often manifesting as cancer, IBS and a host of other chronic illnesses and pain syndromes which can not be otherwise explained.
At The Trauma Recovery Institute We Endeavour

- to co-create an interpersonally synchronized right brain-to-right brain emotional dialogue beneath the words with clients
- to empathically receive the client’s rapid implicit (unconscious) nonverbal communications in synchronized mutual regressions
- to sensitively monitor very slight changes in the other’s emotional expressions
- to intuitively track physiological variations in the patient’s emotional prosody, facial expressions, and gestures
- to interoceptively read one’s own physiological autonomic responses to the client’s emotional communications
- to transiently shift from the verbal left into the nonverbal right brain and the deeper core of the personality
- to co-create a relational context of implicit safety and trust with the client
- to be able to work with strong, traumatic affect and relational trauma, typically found in personality and psychiatric disorders
- to engage in stressful dyadic transference-countertransference and rupture and repair transactions
- to be intuitively aware of one’s own spontaneous bodily-based subjective and intersubjective experience
- to offer well-timed interventions and interpretations that can impact the client’s unconscious levels
- to interactively regulate the patient’s dysregulated affective states, across a spectrum of psychopathologies.
At The Trauma Recovery Institute We Focus
on how to work more directly and effectively with bodily-based emotions, unconscious affect and transference – countertransference within the therapeutic relationship, especially in “heightened affective moments” of the session. Attention is also placed upon working with the defenses of right brain dissociation and left brain repression that blot out strong emotions from consciousness. This central focus on right (and not left) brain affect regulation in the co-created psychotherapy relationship shifts the clinical focus from a reasoned, coherent cognitive narrative to a spontaneous emotion-laden conversation. In this manner the clinical emphasis moves from objective cognitive insight to the subjective change mechanisms embedded in the emotional attachment bond of the therapeutic relationship itself. Trauma Recovery is a complex pursuit and due to trauma and neglect’s impact on all bodily systems, any approach to address the presenting symptoms will be an oversimplified model, therefore we must approach trauma with a multidisciplinary approach on top of cultivating presence and establishing a strong therapeutic alliance with our clients. Modules of treatments such as SE, EMDR, Neurofeedback etc may be helpful adjuncts but they are way too simplified to be effective treatment for trauma, complex trauma and the presenting symptoms of trauma and neglect.
The right brain implicit self represents the biological substrate of the human unconscious mind and is intimately involved in the processing of bodily based affective information associated with various motivational states. The survival functions of the right hemisphere, the lo- cus of the emotional brain, are dominant in relational contexts at all stages of the lifespan, including the intimate context of psychotherapy. The central focus of the psychotherapeutic encounter is to appreciate the client’s motivation, we need to discern the emotional experience he or she seeks. At times, the goal sought will be self- evident to client and [therapist]. At other times, the goal will lie out of awareness and will be difficult to ascertain. The golden thread in assessing motivation lies in discovering the affect being sought in conjunction with the behavior being investigated. In other words, understanding the need underpinning the behaviour, the corrective emotional experience so to speak. The right hemisphere is dominant for the recognition of emotions, the expression of spontaneous and intense emotions, and the nonverbal communication of emotions. The central role of this hemisphere in survival functions is that the right hemisphere operates a distributed network for rapid responding to danger and other urgent problems. It preferentially processes environ- mental challenge, stress and pain and manages self-protective responses such as avoidance and escape. Emotionality is thus the right brain’s “red phone,” compelling the mind to handle urgent matters without delay. Neurobiological studies also demonstrate that the right cortical hemisphere is centrally involved in “the processing of self-images, at least when self-images are not consciously perceived. Deep psychotherapeutic changes alter not only conscious but unconscious self-image associated with nonconscious internal working models of attachment. Both unconscious negative emotions and unconscious self-images are important elements of the psychotherapy process, especially with the more severe self pathologies. Thus, the essential roles of the right brain in the unconscious processing of emotional stimuli and in emotional communication are directly relevant to recent clinical models of an affective unconscious and a relational unconscious, whereby one unconscious mind communicates with another unconscious mind such at that with the therapeutic alliance.


Interactive psychobiological regulation provides the relational context under which the client can safely contact, describe and eventually regulate inner experience. It is the client's experience of empowering action in the context of safety provided by a background of the empathic clinician's psychobiologically attuned interactive affect regulation that helps effect change. This form of presence to right brain affect regulation is critical for change process in psychotherapy.
The Trauma Recovery Institute
The Neurophysiology of Trauma & Threat
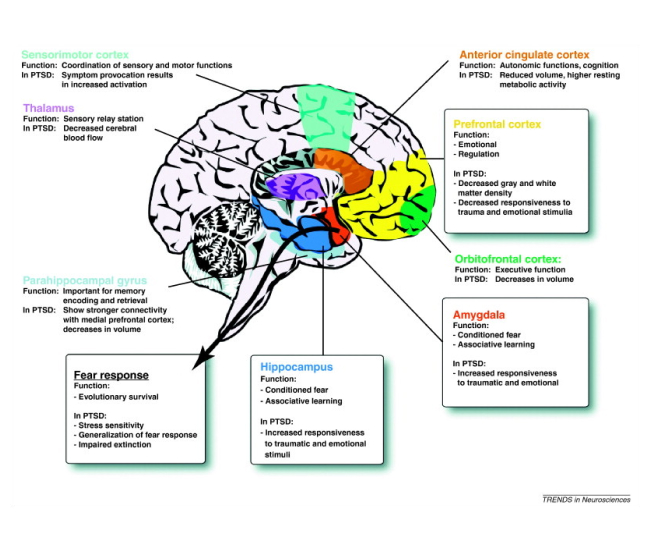
The frontal and central areas of the right cerebral hemisphere are the regions in the brain which attend to the arousal response and to threatening information. The parts of the brain that function in an executive fashion (e.g. thinking, planning, communicating, using any type of rational thought) are, in general, not essential for the execution of emergency behavior. Typically, the first level of information that warns us of an impending threat is accessed and received by the primary senses (smell, vision and hearing). Messages from these basic senses are routed to the locus ceruleus or blue center - a tiny cluster of cells in the brainstem. The locus ceruleus sends the message on the the amygdala (the ‘olive’) which is the center for memory of emotionally laden information. Because of its function as the storehouse and processor of emotionally charged experiences, the amygdala plays a crucial role in the mediation of the response to a perceived / conditioned threat experience. Therefore, any part of the brain receiving information which has been processed by the amygdala is likely to be influenced significantly by the emotional conditioning attached to the threat experience. The amygdala then sends messages tot the hippocampus (the ‘sea horse’), as well as to other parts of the brain. The hippocampus forms a conscious structure for the threat-based message that includes its emotional / conditioned importance, and then sends it on to the orbitofrontal cortex, the master regulator of survival behavior (both conscious and unconscious). The orbitofrontal cortex then sends information to many parts of the brain which may then organize and initiate the necessary behavior patterns which can help the individual survive. It also activates the body’s endocrine response through the hypothalamic / pituitary / adrenal (HPA) axis. The hypothalamus is a center deep in the middle and base of the brain. In addition to regulating many other complex functions (e.g. sleep and appetite), it also regulates the autonomic nervous system. In the case of a threat, the sympathetic nervous system (the energy-burning survival part) is activated. The pituitary gland (the master endocrine gland) is also activated and initiates the body’s endocrine response. The pituitary gland, through the hormone adrenocorticotropic homone (ACTH) stimulates the adrenal glands to release cortisol, which puts a brake on norepinephrine - thus modulating the brain’s arousal response.In the event that the individual survives the immediate threat, cortisol also prepares the animal to manage ongoing stress through changes in its circulation, metabolism, and immune responses. This complex interaction of nerve centers, glands, and chemicals is typical of the multiple interactive feedback systems by which the body is designed to not only survive a threatening event, but also to regulate itself and to promote stability of the entire organism.
Fight, Fright, Freeze Response
All animals must have the capacity to learn from life-threatening experiences. All animals learn to survive through the functions of the areas of the brain that process information through a complex behavioral process that has been termed ‘ the fight / flight / freeze response’. The brain pathways and behaviors in this response are common to all animals from reptiles to primates. But these instincts only form a template on which exposure to a series of life threats builds specific survival skills. Whether one fights or flees when exposed to a threat must be learned very quickly through such experiences. The information from these learning experiences must be stored in unconscious form in order to be of use in the survival game. It must be capable of triggering a predictable behavioral response learned through trial and error without thinking or planning. The process through which we learn these survival skills is called classical conditioning, a term coined by Pavlov (1926). All threatening experiences, even those that are successfully resolved, will prompt unconscious responses related to cues from that experience. Persistence of the conditioned response to the conditioned stimulus is dependent on reinforcement. The internal or external repetition of the traumatic event (or events of a similar kind) will deliver such reinforcement. The process of classical conditioning involves intrinsic or unconscious memory, part of which is ‘procedural memory’ (the part that we use to learn skills). Survival depends upon classical conditioning through procedural memory. The capacity to initiate the fight / flight response is determined by the sympathetic nervous system - one of the two branches of the autonomic nervous system. The sympathetic nervous system is responsible for activating the cardiovascular and motor systems of the body and for making available the extra energy for the vigorous physical activity required to fight or flee.
The Freeze Response
Sometimes fight or flight options are no longer available. Under these circumstances a third survival option is available: the freeze response. The freeze response, common to all species, indeed may allow the animal to survive, but in mammals it sometimes comes at a terrible cost. Animals who survive the freeze response experience an unconscious ‘discharge’ of all of the energy and stored memories of the threat and failed escape through stereotyped body movements as the animal ‘awakens’. If they don’t experience this discharge, a host of adverse behavioral and health problems may follow. Classical conditioning in this context can fool the brain and lead to a host of inappropriate and ineffectual survival behaviors. When this happens we may say that ‘trauma’ has occurred. When fight or flight are unsuccessful or not possible, a third instinctual and quite unconscious option will be exercised. The animal collapses and becomes immobile. This is the freeze response. If the freeze response is successful in preventing the animal from being killed, the animal will gradually emerge from immobility. The freeze response is made possible through the functioning of the parasympathetic nervous system. When the parasympathetic response is very strong or extreme, the animal in freeze is in a precarious state of abnormally dysregulated and fluctuating autonomic nervous system activity. One of the expressions of the freeze response in humans is the phenomenon of dissociation. Dissociation is reflective of a state of shock, stunning, trance, numbing of emotion and cognitive fogging. Dissociation is physiologically the same as the freeze. Research suggests that PTSD patients experience a dramatic reduction of many of their symptoms when they were allowed to complete the motor discharge of their freeze response through unique therapeutic behavioral techniques. In the absence of of this freeze discharge, the ‘energy’ of the intense arousal associated with the threat and attempted escape remains bound in the body and brain, leading to a host of abnormal symptoms that we attribute to PTSD. Research and clinical observations also suggests that repeated freeze events without discharge seemed to be cumulative, adding to a progressive worsening of post-traumatic symptoms and to the development of progressive helplessness in the face of threat.
Signs & Symptoms
How Do I know If I Have Trauma
Intimacy
Fear of or avoidance of intimate relationships. This can often be masked with religiosity, spiritual bypassing, pursuit of activities, success, money and career which leave no time or space for meaningful relationships.
Relational Difficulties
Difficulties with resolving conflicts in relationships. Quick to anger or withdrawal when there is a disagreement. Hypersensitive to perceptions of rejection, abandonment and loss of love.
Ongoing Health Challenges
Metabolic disease states such as diabetes, cancer and heart disease are often rooted in childhood trauma & neglect. This is true also for a group of health challenges under autoimmunity such as IBD and CFS.
PTSD
Experiences of intense fear, terror & anxiety. A difficulty feeling safe. Experiences of flashbacks. Difficulty sleeping. Often feeling dissociated.
Addictions
Addictions to sugar, alcohol, drugs, junk foods, sex, work, gambling, devices, social media, gaming etc
Emotions
Difficulty with naming, connecting to and expressing to others your feelings. Which we call Alexithymia.
Sense of Self
Feelings of shame, guilt and self hatred. Critical of self. Compassion towards others but not towards self which we call chronic compassion. Difficulties with identity.
Depression
Lack of life force energy, lack of sexual energy. Frequent states of low mood, energy and appetite. Clinical depression effecting functionality. Feelings of hopelessness and loss of interest in life.
Talk therapy alone is not enough to address deep rooted trauma that may be stuck in the body, we need also to engage the body in the therapeutic process and engage ourselves as therapists and clients to a complex interrelational therapeutic dyad addressing transference - countertransferential modes of communication, rupture and repair, right brain to right brain, limbic system to limbic system, in order to address and explore trauma that persists in our bodies as adults which can present as complex reenactments inside and outside of therapy and influences our adult relationships, thinking and behaviour.
The Trauma Recovery Institute
Adverse Childhood Experiences (ACEs) - The Ace Study

“To Exist is to Change, To change is to Mature, To mature is to go on creating one’s self endlessly – Henri Bergson
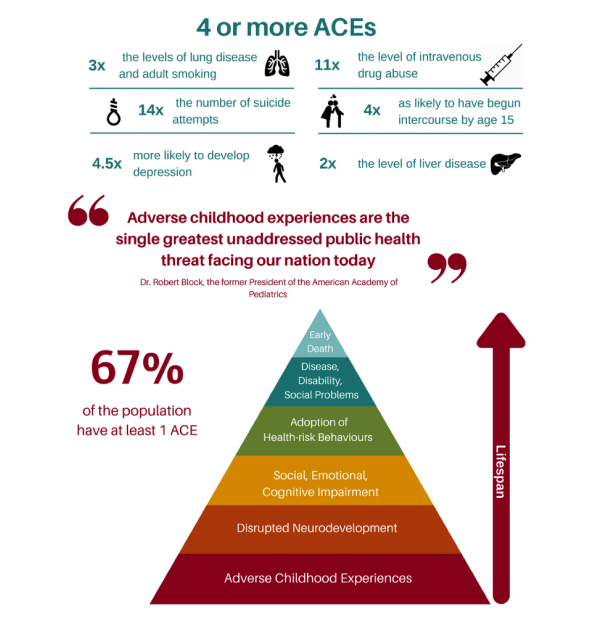
Adverse Childhood Experiences study is a groundbreaking study conducted in 1995 by the Centers for Disease Control and the Kaiser Permanente health care organization in California. In that study, “ACEs” referred to three specific kinds of adversity children faced in the home environment—various forms of physical and emotional abuse, neglect, and household dysfunction. The key findings of dozens of studies using the original ACEs data are: (1) ACEs are quite common, even among a middle-class population: more than two-thirds of the population report experiencing one ACE, and nearly a quarter have experienced three or more. (2) There is a powerful, persistent correlation between the more ACEs experienced and the greater the chance of poor outcomes later in life, including dramatically increased risk of heart disease, diabetes, obesity, depression, substance abuse, smoking, poor academic achievement, time out of work, and early death. ACEs research shows the correlation between early adversity and poor outcomes later in life. Toxic stress explains how ACEs ”get under the skin” and trigger biological reactions that lead to those outcomes.
In the early 2000s, the National Scientific Council on the Developing Child coined the term “toxic stress” to describe extensive, scientific knowledge about the effects of excessive activation of stress response systems on a child’s developing brain, as well as the immune system, metabolic regulatory systems, and cardiovascular system. Experiencing ACEs triggers all of these interacting stress response systems. When a child experiences multiple ACEs over time—especially without supportive relationships with adults to provide buffering protection—the experiences will trigger an excessive and long-lasting stress response, which can have a wear-and-tear effect on the body, like revving a car engine for days or weeks at a time. Importantly, the Council also expanded its definition of adversity beyond the categories that were the focus of the initial ACE study to include community and systemic causes—such as violence in the child’s community and experiences with racism and chronic poverty—because the body’s stress response does not distinguish between overt threats from inside or outside the home environment, it just recognizes when there is a threat, and goes on high alert. While trauma has many definitions, typically in psychology it refers to an experience of serious adversity or terror—or the emotional or psychological response to that experience. Trauma-informed care or services are characterized by an understanding that problematic behaviors may need to be treated as a result of the ACEs or other traumatic experiences someone has had, as opposed to addressing them as simply willful and/or punishable actions.
Damasio said that we hide the truth of the adversity we experience below conscious awareness, the price of this is that we must then act it out, which can be through rage, addictions, anti social behaviour, narcissistic attitudes etc this behaviour we witness by some of those we love as unpleasant as it may be is often a cry for help, this behaviour is a defence protecting a very wounded part of ourselves. Remember all behaviour is communication, we must ask what is been communicated.
The Trauma Recovery Institute
Attachment relationships have a fundamental impact on the developing infant. Over the last two decades, methodological and technological advances in neuroscience have provided us with hugely enlightening insights into how our attachment history shapes and structures the brain. It has highlighted how and why, integration of the brain structures is necessary for optimal psychological health. Neural integration brings with it the ease of well-being; without it, we now know, physical neuronal firing can be constrained by past synaptic learning, which creates behavioural patterns, and engrained, sometimes chaotic, emotional responses (Siegel, 2010). Trauma and Neglect can be framed as events in childhood that should not have happened and events which should have happened but did not. Attachment is a special emotional relationship that involves an exchange of comfort, care, and pleasure. Attachment is a relationship in the service of a baby’s emotion regulation and exploration. It is the deep, abiding confidence a baby has in the availability and responsiveness of the caregiver. Attachment is about creating a safe environment for optimal brain development for the child of which non stressed consistent attuned caregiving, touch, play, laughter, meeting basic needs and positive affirmation are all important parts of. When this goes wrong it has huge implications as we have been discussing in this Section. However the right kind of psychotherapy can correct this and through this therapeutic alliance with a safe therapist gives opportunity to what we call earned secure attachment.

Neglect is Complex Trauma - Often Unrecognised
As you can see from the ACE study, trauma can be much broader than once defined and now we understand the huge psychobiological impact of early abuse and neglect. In fact there is a large population of people who present with trauma symptoms who have never identified themselves of having experienced trauma, most often this is due to the subtle covert experience of childhood neglect, it is hard to know what is missing when you have never experienced that which is missing. Childhood neglect is pervasive and there are a number of forms of neglect including children who grew up in what may have looked like from the outside as healthy, wealthy and functional families when fact the child have have experienced proximal abandonment which is a term to describe when parents are there but not really there, not in the attuned way that is necessary for optimal development. Another form of neglect and complex trauma is covert incest which is a parental attachment style that is invasive, where the parent gets their needs met from the child giving the child a huge amount of non age appropriate responsibility, thus setting up a role reversal and most often comes at the expense of play and spontaneity. This form of neglect is highly dysregulating for the developing child often showing up as autoimmune disease in adulthood.
We now know that the mother and infant relationship directly shapes maturation of the infant’s right brain (Schore, 1996). This hemisphere has connections to the limbic system and the body and responds non-verbally, emotionally and relationally. The left hemisphere, in contrast, responds linguistically, logically and analytically (Wallin, 2007). Crucially, however, in the first few years of life, the right hemisphere is dominant; thus, early attachment memories are recorded experientially, through face-to-face, body-to-body, right-brain-to-right-brain interactions (Schore, 1996, 2009; Travarthen, 2001). It is the right brain’s pre-linguistic, somato-sensory-motor structures then that store the experience of secure attachment as well as the experience of rejection, abandonment or neglect
Schore
Trauma and the Nervous System
Exposure to extreme threat, particularly early in life, combined with a lack of adequate caregiving responses significantly affect the long-term capacity of the human organism to modulate the response of the sympathetic and parasympathetic nervous systems in response to subsequent stress. The sympathetic nervous system (SNS) is primarily geared to mobilization by preparing the body for action by increasing cardiac output, stimulating sweat glands, and by inhibiting the gastrointestinal tract. Since the SNS has long been associated with emotion, a great deal of work on the role of the SNS has been collected to identify autonomic “signatures” of specific affective states. Overall, increased adrenergic activity is found in about two-thirds of traumatized children and adults. The parasympathetic branch of the ANS not only influences HR independently of the sympathetic branch, but makes a greater contribution to HR, including resting HR. Vagal fibers originating in the brainstem affect emotional and behavioral responses to stress by inhibiting sympathetic influence to the sinoatrial node and promoting rapid decreases in metabolic output that enable almost instantaneous shifts in behavioral state. The parasympathetic system consists of two branches: the ventral vagal complex (VVC) and the dorsal vagal complex (DVC) systems. The DVC is primarily associated with digestive, taste, and hypoxic responses in mammals. The DVC contributes to pathophysiological conditions including the formation of ulcers via excess gastric secretion and colitis. In contrast, the VVC has the primary control of supradiaphragmatic visceral organs including the larynx, pharynx, bronchi, esophagus, and heart. The VVC inhibits the mobilization of the SNS, enabling rapid engagement and disengagement in the environment.
The Dorsal Vagal State and Manifestation of Autoimmune Disorders
People who are in the dorsal vagal state a lot which is the state when the amygdala is activated due to a detection of a slight threat in the environment consciously or unconsciously through neuroception and the traumatized person goes into a state of learned helplessness or what is called dissociation or freeze response which is an unconscious conditioned fear response, the body’s reflex to an internal or external stimuli from a cue of an original trauma. This will activate all the viscera, your heart, your lungs, your colon, your stomach, all of these are run unconsciously by the dorsal vagal nucleus and if you have syndromes where you are in the freeze response a lot, the dorsal vagal nucleus will be hyperactive and you will get syndromes of hyperactivity within the viscera and that can be characterized by Irritable bowel disease, colitis and other autoimmune diseases.
These are cyclical diseases which means they oscillate between sympathetic and parasympathetic nervous system meaning the symptoms come and go which is why the medical profession very often can not diagnose the problem or refer to it as psychosomatic meaning it is a condition of the mind when in fact it is actually emotionally driven physiological conditions of the gut and the brain. Problems with the gut are common with people who have had trauma, it is the physiology of trauma that drives these conditions and so if you heal the trauma you can heal the disease. These conditions are also referred to as neurosomatic, which means they are brain based conditions, physical conditions caused by abnormal function of the brain.
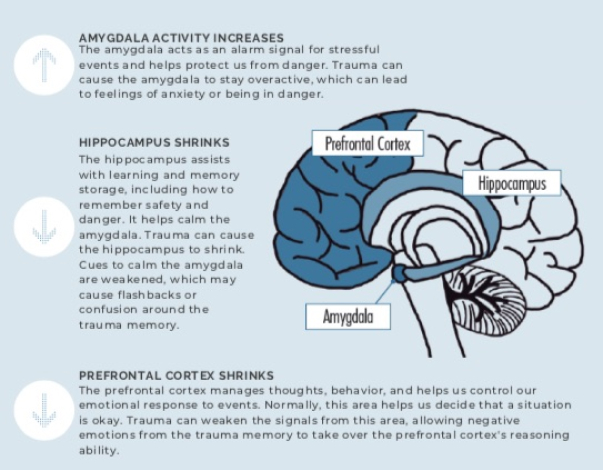
The Amygdala is the agent of fear conditioning, it stores emotionally based memory positive and negative, it is also the gate keeper for responding to threat by activating the fight or flight response, when the fight or flight response is not successful, such as you can not escape the traumatic event, the body goes into a freeze response. The freeze response is predicated by the effects of early childhood experiences, the freeze response is also called dissociation. When dissociation happens you are dysregulated, Dissociation is based a lot on what happened in childhood that allowed you to develop the brain in a way to prevent that from happening too easy. This has to do with Allan Schore’s work on attunement, the part of the brain that controls this regulation of autonomic nervous system and emotional system, which is the orbital frontal cortex. This develops in a healthy attuned infant and shrinks in a neglected infant. We need a developed orbital frontal cortex to regulate us over our lifetime and prevent us from going into freeze states and dysregulation. Helplessness is the essential ingredient for the freeze response.
The freeze response is a motor action, which perpetuates the escape behaviour in a way that erases all the procedural (Implicit) memory of that trauma. If you have a threat and don’t discharge the freeze response, you are conditioned thereafter to any body cues related to that traumatic event.